The ultrasound images are shown below:




What is that? We'll discuss in detail.
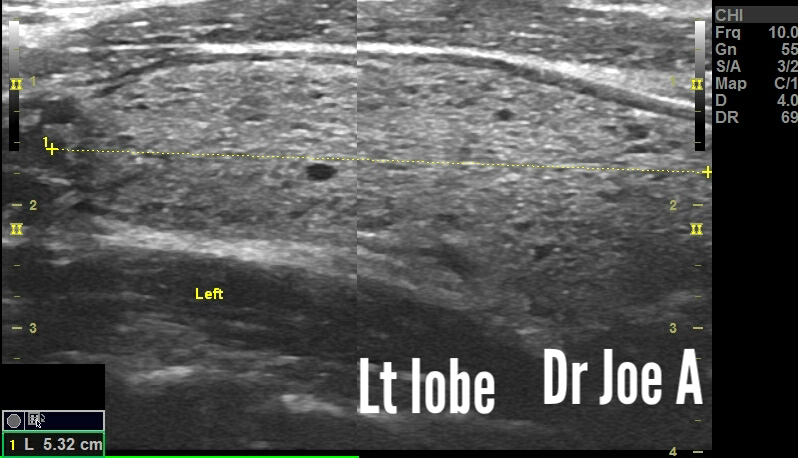
What is unusual is that it is rather prominent in this case.
Final diagnosis: a prominent falciform ligament in the liver.
Located at the junction between the right and left lobes of liver.
Why do I think this is the falciform ligament?
An echogenic vertical band between the right and left lobes of the liver in an adult male is most likely the falciform ligament. The falciform ligament is a fibrous band of tissue that separates the right and left lobes of the liver. It is made up of connective tissue and contains a small amount of fat.
Significance:
The falciform ligament is a normal finding and does not usually cause any problems.
Can it be abnormal?
In some cases, an echogenic vertical band between the right and left lobes of the liver can be a sign of a more serious condition, such as a liver tumor or a liver abscess. However, these conditions are rare and would usually be accompanied by other symptoms, such as pain, fever, and jaundice.
Here are some additional details about the falciform ligament:
* It is a thin, fibrous band of tissue that extends from the diaphragm to the umbilicus.
* It separates the right and left lobes of the liver.
* It contains a small amount of fat.
* It is a normal finding and does not usually cause any problems.
More facts about the falciform ligament:
It is usually less than 1 cm thick.
In some cases, the falciform ligament may appear thickened or irregular. This may be due to a number of conditions, including:
* Liver disease, such as cirrhosis or hepatitis
* Inflammation of the falciform ligament (falciform ligamentitis)
* A tumor or abscess in the liver
* A blood clot in the falciform ligament (thrombus)
Here are some of the reasons why the falciform ligament may be prominent or visible as in this case:
1. Body habitus: The falciform ligament is more likely to be visible in thin patients. This is because the ligament is more superficial and easier to see.
2. Abnormalities in the liver: The falciform ligament may be more prominent if there is an abnormality in the liver, such as a cyst or tumor. This is because the ligament may be stretched or compressed by the abnormality.
3.Technique: The falciform ligament may be more visible if the ultrasound technician is using a high-frequency probe and is scanning in the right plane
If the falciform ligament appears thickened or irregular on ultrasound imaging, it may be advisable to have additional tests, such as a CT scan or MRI, to determine the cause.
A word on another important ligament that may be visible in some cases: The ligament teres:
The ligamentum teres is a fibrous cord that is located in the free, inferior border of the falciform ligament. It is a remnant of the umbilical vein, which carried blood from the placenta to the fetus during pregnancy. The ligamentum teres courses along a fissure situated between the inferior surface of the right and left lobes of the liver. It can be seen on ultrasound as a thin, linear structure that runs parallel to the falciform ligament.
The ligamentum teres is not always visible on ultrasound. This is because it can be small and/or fatty. It is more likely to be visible in people who have had surgery on their abdomen, such as a cesarean section.
The ligamentum teres can be a useful landmark for radiologists and surgeons. It can be used to help identify the liver and its lobes, as well as the falciform ligament. It can also be used to guide needle biopsies of the liver.
Some additional details about the ligamentum teres:
* It is typically about 10-15 cm long.
* It is located in the free, inferior border of the falciform ligament.
* It courses along a fissure situated between the inferior surface of the right and left lobes of the liver.
* It is a remnant of the umbilical vein.
* It is not always visible on ultrasound.
* It can be a useful landmark for radiologists and surgeons.
For more visit: