An ultrasound scan of a male patient with infertility and azoospermia revealed the following:
Description of Ultrasound Imaging Findings
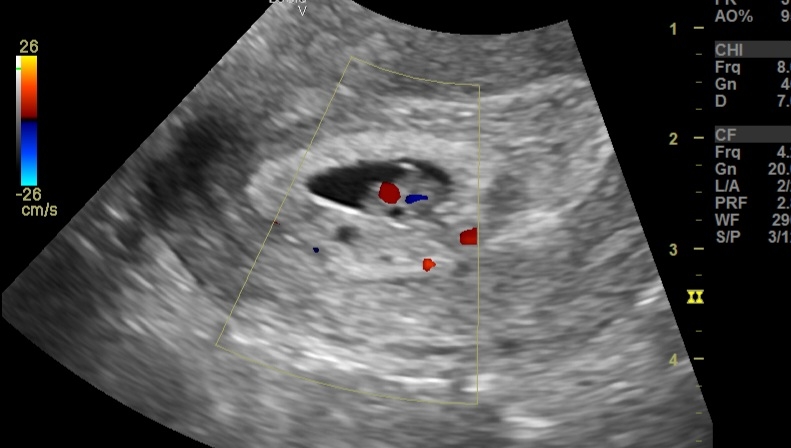
1. Testes:
Small testes with volume <2 cc, significantly below the normal range (12–25 cc).
Poor vascularity on color Doppler, indicating reduced blood flow.
2. Bilateral Grade 1 Varicocele:
Mild dilation of the pampiniform plexus.
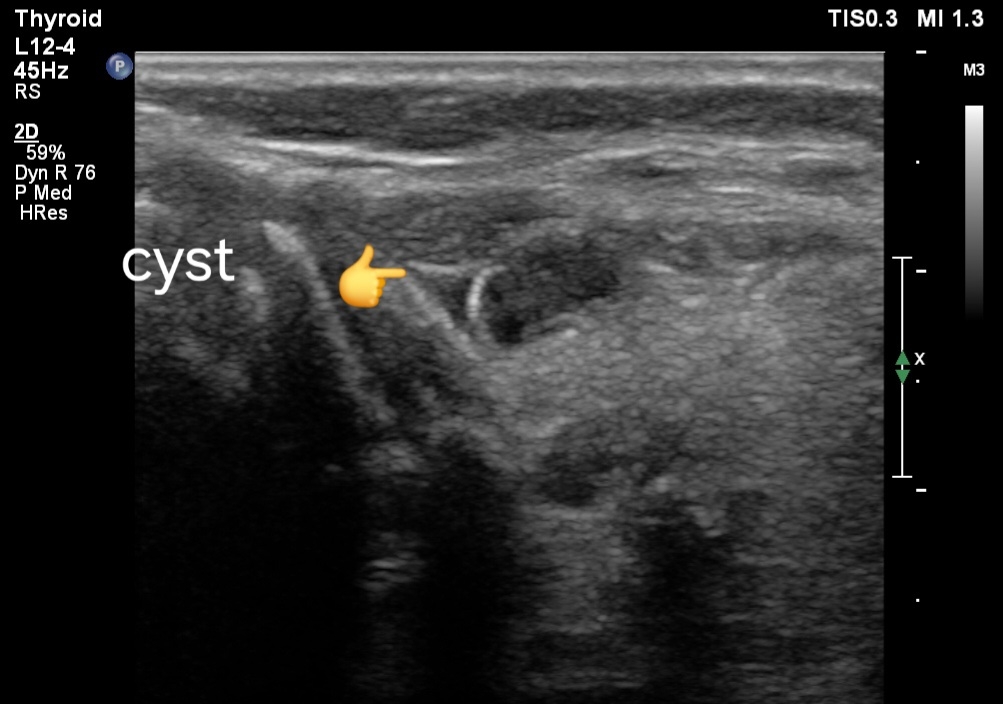
3. Transrectal Ultrasound (TRUS):
Small seminal vesicles, potentially hypoplastic.
Possibly absent vas deferens, indicated by its non-visualization.
Normal prostate with no abnormalities detected.
Differential Diagnoses:
1. Congenital Bilateral Absence of the Vas Deferens (CBAVD):
Commonly associated with cystic fibrosis transmembrane conductance regulator (CFTR) gene mutations.
May present with hypoplastic or absent seminal vesicles and azoospermia.
2. Primary Testicular Failure (Hypogonadism):
Testicular atrophy and poor vascularity may indicate failure of spermatogenesis.
Causes include genetic syndromes like Klinefelter syndrome, previous orchitis, or trauma.
3. Y-Chromosome Microdeletions:
Specifically in the AZF region, leading to testicular dysfunction and azoospermia.
4. Obstructive Azoospermia:
Secondary to structural anomalies like CBAVD or scarring.
5. Secondary Hypogonadism:
If associated with pituitary or hypothalamic dysfunction, but this is less likely given the absent vas deferens.
---
Most Likely Diagnosis
Congenital Bilateral Absence of the Vas Deferens (CBAVD):
The combination of small testes, poorly vascular testes, azoospermia, small seminal vesicles, and absent vas deferens strongly suggests CBAVD.
---
Prognosis
Fertility:
Natural conception is not possible.
Sperm retrieval techniques (e.g., testicular sperm extraction, TESE) combined with intracytoplasmic sperm injection (ICSI) may be viable for fathering biological children.
Overall Health:
Usually, no systemic health effects unless associated with CFTR mutations.
If CFTR-related, patients may have subclinical or overt cystic fibrosis symptoms (e.g., recurrent respiratory infections, pancreatitis).
---
Management
1. Diagnostic Confirmation:
Genetic testing for CFTR mutations and Y-chromosome microdeletions.
Hormonal evaluation (FSH, LH, testosterone) to differentiate primary vs. secondary causes.
2. Fertility Options:
Referral to a fertility specialist.
Consideration of TESE with ICSI.
Partner evaluation for CFTR carrier status if CFTR mutation is confirmed.
3. Counseling:
Address psychological and emotional aspects of azoospermia.
Genetic counseling if hereditary factors are identified.
4. Monitoring:
Regular follow-ups for any complications or related health concerns (e.g., cystic fibrosis symptoms).
#Azoospermia
#TesticularHypoplasia
#CBAVD
#MaleInfertility
#UltrasoundDiagnosis
#ReproductiveHealth
#FertilityCare